Pelviureteric Junction Obstruction
Pelviureteric junction (PUJ) obstruction is a restriction to the flow of urine from the renal pelvis to the ureter, which if left uncorrected, may lead to progressive renal deterioration. The blockage is always partial but the degree of a block may vary from minimal to severe. Mild cases usually don’t impair kidney function. Severe cases can cause significant impairment in kidney function. Because it impedes the flow of urine, there is resulting enlargement of the renal pelvis (hydronephrosis). Most often PUJO is congenital (present from birth), usually because of an abnormality in the development of the muscle surrounding the PUJO.
What is Pelviureteric Junction Obstruction?
Pelviureteric junction (PUJ) obstruction is a restriction to the flow of urine from the renal pelvis to the ureter, which if left uncorrected, may lead to progressive renal deterioration. The blockage is always partial but the degree of a block may vary from minimal to severe. Mild cases usually don’t impair kidney function. Severe cases can cause significant impairment in kidney function. Because it impedes the flow of urine, there is resulting enlargement of the renal pelvis (hydronephrosis).
PUJ obstruction (PUJO) is the most common cause (48%) of significant hydronephrosis detected on prenatal ultrasound or in newborns.
What Causes PUJO?
Most often PUJO is congenital (present from birth), usually because of an abnormality in the development of the muscle surrounding the PUJ. PUJO can also occur later in life and can be caused by other factors, including compression of the ureter by abnormal blood vessels, inflammation, stones, or scar tissue.
What are the symptoms of PUJO?
Most infants (less than 1 year) are asymptomatic and most children are discovered because of their symptoms. Symptoms suggesting PUJO include hematuria (blood in the urine), urinary tract infection (UTI), kidney stones, failure to thrive, pain associated with nausea and vomiting, abdominal fullness/palpable mass or hypertension.
What tests are required to confirm the diagnosis?
Due to the increased use of antenatal ultrasound (during pregnancy), if any hydronephrosis is identified, the fetus will need to be monitored throughout the pregnancy. Once the baby is born, a repeat ultrasound is to be done at least a week after delivery to confirm the PUJO.
If PUJO is affecting one kidney, then further investigations can be done when the infant is 4-6 weeks of age. These tests would include blood and urine tests to find out overall kidney function and to rule out UTI.
If both the kidneys are affected by PUJO, your Urologist may get blood and urine tests at the earliest to know the status of overall kidney function. Further course would be decided based on these reports and other details on ultrasound.
A nuclear scan (DTPA /EC renogram) uses a radioactive isotope which is injected intravenously (IV) and this isotope is taken up by the kidneys and excreted in urine. Using a special camera, images of the kidneys can be seen clearly. This test gives information about individual kidney function as well as a degree of blockage. This test can be done above the age of 4- 6 weeks.
CT scans are rarely required to confirm this condition and is also avoided as this involves higher radiation.
Do all cases of PUJO need surgery?
Following are some of the common indications:
•Presence of symptoms (noted above) associated with the obstruction.
•Impairment of overall renal function.
•Progressive impairment of obstructed kidney function.
•Development of stones or infection, or causal hypertension.
What is the goal of correcting this condition surgically?
The aim is to Restore non-obstructed urinary flow. The primary goal of surgery is relief of symptoms and preservation or improvement of renal function.
What is the surgical procedure most commonly performed for this condition?
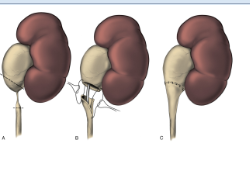
Pyeloplasty is a surgical procedure that removes the scar
tissue from the blocked area and reconnects the healthy part of the ureter
to the renal pelvis, so as to create a wide opening. The
success rate is higher than 95%. Most of the time, open
surgery is performed in infants. In older children and adults the same
procedure can be performed laparoscopically (key hole surgery).
A tube called ureteric stent is usually placed to drain
urine from the operated kidney across the area of repair to the bladder. In
addition, you may have a bladder drainage tube (urethral catheter). Rarely a
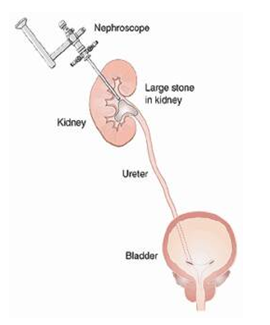
nephrostomy tube (the inner end in the kidney and coming out of a separate
small incision in the flank region) is required to drain the kidney (this is
done when placement of ureteric stent was not possible). Sometimes a drain
tube is placed around the area of repair (outside the kidney), to drain any
blood/urine collection.
What are the do’s and don’ts after this surgery?
You can have a regular diet, once you are able to tolerate orally. Sometimes, especially infants will have swelling of the tummy (abdomen) and this subsides in a day or two, till then IV fluids would be continued. The urethral catheter is usually removed on the 3rd day morning after surgery. And you will be allowed to go home later that evening with ureteric stent (not visible outside the body), if you are doing well.
Drain tube or nephrostomy tube, if placed, would be removed at appropriate times based on the clinical situation. With ureteric stent inside, you may experience urgency, frequency, burning urination, mild blood-tinged urine and flank pain for a minute or so when you are passing urine. These are expected things, but if you have severe pain or high-grade fever, do contact your doctor. You will need to repeat urine culture 2 weeks after surgery. Based on the report, ureteric stent removal would be planned, if required under cover of appropriate antibiotics based on sensitivity.
What are the possible complications that can arise if this condition is left untreated?
If left untreated, PUJ obstruction can lead to progressive loss of kidney function, kidney stones or infection.
What is the follow up after stent removal?
Renal ultrasound is obtained 3 months after pyeloplasty to ensure that the hydronephrosis is reduced or at least remaining stable. A nuclear scan (DTPA / EC) may be obtained 1 year after the pyeloplasty to provide a relative assessment of the overall renal function and drainage pattern.
When do you say surgery is successful?
Improvement in hydronephrosis on ultrasound and stabilization or improvement in function on nuclear scan (DTPA/EC). If patient had symptomatic presentation, resolution of flank/abdominal pain or vomiting should also occur.
What are the other complications of surgery?
Less than 5% of patients may have a recurrence of narrowing at the PUJ requiring redo surgery. Urinary leakage from the area of surgery may require placement of the percutaneous drain. Other problems include wound infection and hernia which are very rare.